
Understanding the Mechanisms of Spinal Neuromodulation Video
Highlighted Papers
Coming Soon!
Cervical transcutaneous spinal stimulation for spinal motor mapping
Jeonghoon Oh, Alexander G. Steele, Blesson Varghese, Catherine A. Martin, Michelle S. Scheffler, Rachel L. Markley, Yi-KaiLo, Dimitry G. Sayenko
iScience Journal
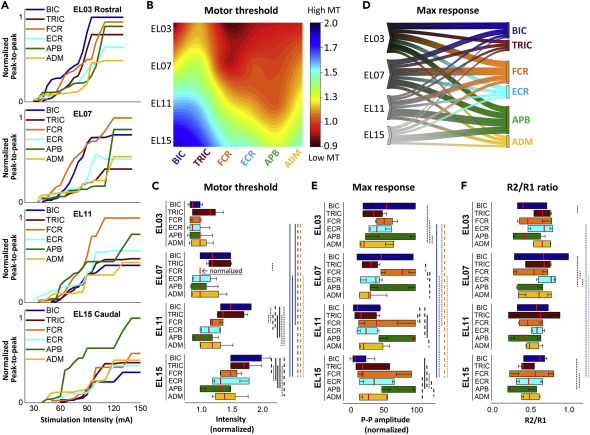
Transcutaneous spinal stimulation (TSS) is a promising approach to restore upper-limb (UL) functions after spinal cord injury (SCI) in humans. We sought to demonstrate the selectivity of recruitment of individual UL motor pools during cervical TSS using different electrode placements. We demonstrated that TSS delivered over the rostrocaudal and mediolateral axes of the cervical spine resulted in a preferential activation of proximal, distal, and ipsilateral UL muscles. This was revealed by changes in motor threshold intensity, maximum amplitude, and the amount of post-activation depression of the evoked responses. We propose that an arrangement of electrodes targeting specific UL motor pools may result in superior efficacy, restoring more diverse motor activities after neurological injuries and disorders, including severe SCI.
Characterization of spinal sensorimotor network using transcutaneous spinal stimulation during voluntary movement preparation and performance
Alexander G Steele, Darryn A Atkinson, Blesson Varghese, Jeonghoon Oh, Rachel L Markley, Dimitry G Sayenko
Journal of Clinical Medicine
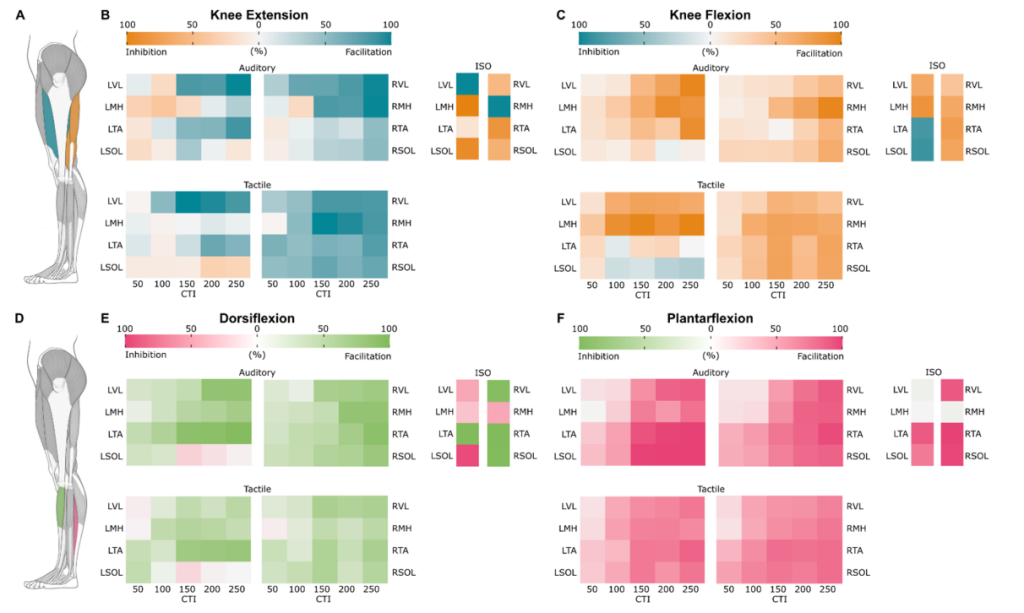
Transcutaneous electrical spinal stimulation (TSS) can be used to selectively activate motor pools based on their anatomical arrangements in the lumbosacral enlargement. These spatial patterns of spinal motor activation may have important clinical implications, especially when there is a need to target specific muscle groups. However, our understanding of the net effects and interplay between the motor pools projecting to agonist and antagonist muscles during the preparation and performance of voluntary movements is still limited. The present study was designed to systematically investigate and differentiate the multi-segmental convergence of supraspinal inputs on the lumbosacral neural network before and during the execution of voluntary leg movements in neurologically intact participants. During the experiments, participants (N = 13) performed isometric (1) knee flexion and (2) extension, as well as (3) plantarflexion and (4) dorsiflexion. TSS consisting of a pair pulse with 50 ms interstimulus interval was delivered over the T12-L1 vertebrae during the muscle contractions, as well as within 50 to 250 ms following the auditory or tactile stimuli, to characterize the temporal profiles of net spinal motor output during movement preparation. Facilitation of evoked motor potentials in the ipsilateral agonists and contralateral antagonists emerged as early as 50 ms following the cue and increased prior to movement onset. These results suggest that the descending drive modulates the activity of the inter-neuronal circuitry within spinal sensorimotor networks in specific, functionally relevant spatiotemporal patterns, which has a direct implication for the characterization of the state of those networks in individuals with neurological conditions.
Statistics
All Papers
Objective: The objective of this narrative review was to locate and assess recent articles employing a combinatorial approach of transcutaneous spinal cord stimulation or epidural spinal cord stimulation with additional modalities. We sought to provide relevant knowledge of recent literature and advance understanding on outcomes reported, to better equip those working in neurorehabilitation and neuromodulation. Methods: Articles were selected and analyzed based on study approach, stimulation parameters, outcome measures, and presence of neurophysiological data to support findings. Results: This narrative review analyzed 44 recent articles employing a combinatorial approach of transcutaneous spinal cord stimulation or epidural spinal cord stimulation with additional modalities. Our findings showed that limited research exists regarding such combinatorial approaches, particularly when considering modalities beyond activity-based training. There is also limited consistency in neurophysiological and quality of life outcomes. Conclusion: Articles involving transcutaneous spinal cord stimulation or epidural spinal cord stimulation with other modalities are limited in the current body of literature. Authors noted variety in approach, sample size, and use of participant perspective. Opportunities are present to add high quality research to this body of literature. Significance: Transcutaneous spinal cord stimulation and epidural spinal cord stimulation are emerging in research as viable avenues for targeting improvement of function after traumatic spinal cord injury, particularly when combined with activity-based training. This body of literature demonstrates viable areas for growth from both neurophysiological and functional perspectives. Further, exploration of novel combinatorial approaches holds potential to offer enhanced contributions to clinical and neurophysiological rehabilitation and research.
Transcutaneous Spinal Stimulation (TSS) is a non-invasive neuromodulation technique that can alter excitability of spinal sensorimotor network below spinal cord injury (SCI) and facilitate neural circuits regulating rhythm and pattern generation during movements. There has been a surge in research to determine mechanistic and functional benefits of spinal stimulation for individuals with spinal cord injury. TSS can be utilized to target specific limb muscles and enable improved motor activity with functional tasks such as upright posture, reaching, and stepping. We hypothesized that targeted TSS can increase force generation by the lower extremity muscles and improve synergistic muscle activation during stepping. TSS has the potential to be individually tailored/delivered to promote specific motor tasks but requires systematic exploration of responses. Continuous stimulation is currently the standard TSS technique reported in recent research and demonstrates modest specificity during standing.
Background and Purpose: activities-based locomotor training (AB-LT) is a restorative therapeutic approach to the treatment of movement deficits in people with non-progressive neurological conditions, including cerebral palsy (CP). Transcutaneous spinal stimulation (TSS) is an emerging tool in the rehabilitation of individuals with sensorimotor deficits caused by neurological dysfunction. This non-invasive technique delivers electrical stimulation over the spinal cord, leading to the modulation of spinal sensorimotor networks. TSS has been used in combination with AB-LT and has been shown to improve muscle activation patterns and enhance motor recovery. However, there are no published studies comparing AB-LT + TSS to AB-LT alone in children with CP. The purpose of this case study was to compare the impact of AB-LT alone versus AB-LT combined with TSS on functional movement and quality of life in a child with CP. Methods: A 13-year-old male with quadriplegic CP participated in this pilot study. He was classified in the Gross Motor Function Classification System (GMFCS) at Level III. He completed 20 sessions of AB-LT (5x/week), then a 2-week washout period, followed by 20 sessions of body-AB-LT + TSS. Treatment sessions consisted of 1 h of locomotor training with body weight support and manual facilitation and 30 min of overground play-based activities. TSS was applied using the RTI Xcite®, with stimulation at the T11 and L1 vertebral levels. Assessments including the Gross Motor Function Measure (GMFM), 10-m walk test (10 MWT), and Pediatric Balance Scale (PBS) were performed, while spatiotemporal gait parameters were assessed using the Zeno Walkway®. All assessments were performed at three time points: before and after AB-LT, as well as after AB-LT + TSS. OUTCOMES: After 19/20 sessions of AB-LT alone, the participant showed modest improvements in the GMFM scores (from 86.32 to 88), 10 MWT speed (from 1.05 m/s to 1.1 m/s), and PBS scores (from 40 to 42). Following the AB-LT combined with TSS, scores improved to an even greater extent compared with AB-LT alone, with the GMFM increasing to 93.7, 10 MWT speed to 1.43 m/s, and PBS to 44. The most significant gains were observed in the GMFM and 10 MWT. Additionally, improvements were noted across all spatiotemporal gait parameters, particularly at faster walking speeds. Perhaps most notably, the child transitioned from the GMFCS level III to level II by the end of the study. Discussion: Higher frequency and intensity interventions aimed at promoting neuroplasticity to improve movement quality in children with CP are emerging as a promising alternative to traditional physical therapy approaches. This case study highlights the potential of TSS to augment neuroplasticity-driven treatment approaches, leading to improvements in neuromotor function in children with CP. These findings suggest that TSS could be a valuable addition to rehabilitation strategies, warranting further research to explore its efficacy in larger populations.
Introduction: Spinal cord injury (SCI) animal models often utilize an open surgical laminectomy, which results in animal morbidity and also leads to changes in spinal canal diameter, spinal cord perfusion, cerebrospinal fluid flow dynamics, and spinal stability which may confound SCI research. Moreover, the use of open surgical laminectomy for injury creation lacks realism when considering human SCI scenarios.
Methods: We developed a novel, image-guided, minimally invasive, large animal model of SCI which utilizes a kyphoplasty balloon inserted into the epidural space via an interlaminar approach without the need for open surgery.
Results: The model was validated in 5 Yucatán pigs with imaging, neurofunctional, histologic, and electrophysiologic findings consistent with a mild compression injury.
Discussion: Few large animal models exist that have the potential to reproduce the mechanisms of spinal cord injury (SCI) commonly seen in humans, which in turn limits the relevance and applicability of SCI translational research. SCI research relies heavily on animal models, which typically involve an open surgical, dorsal laminectomy which is inherently invasive and may have untoward consequences on animal morbidity and spinal physiology that limit translational impact. We developed a minimally invasive, large animal model of spinal cord injury which utilizes a kyphoplasty balloon inserted percutaneously into the spinal epidural space. Balloon inflation results in a targeted, compressive spinal cord injury with histological and electrophysiological features directly relevant to human spinal cord injury cases without the need for invasive surgery. Balloon inflation pressure, length of time that balloon remains inflated, and speed of inflation may be modified to achieve variations in injury severity and subtype.
BACKGROUND
Spinal cord stimulation (SCS) has demonstrated potential as a therapy to enhance motor functional recovery after spinal cord injury (SCI). Epidural SCS for motor recovery is traditionally performed via the dorsal electrode. While ventral epidural stimulation may provide more direct and specific stimulation of the ventral motor neurons involved in motor control, it is largely unstudied, and its role in motor recovery after SCI is unclear. In order to profile the safety and feasibility of ventral epidural spinal stimulation (VSS), the authors present a patient who underwent VSS following a corpectomy to treat SCI related to metastatic epidural cord compression.
OBSERVATIONS
A patient underwent transpedicular corpectomy for spinal cord decompression, as well as the placement of 2 ventral epidural electrodes, followed by concurrent physical therapy and ventral epidural stimulation. He was nonambulatory preoperatively but was able to walk over 300 feet with the assistance of a rolling walker at the conclusion of the 3-week study period. VSS was noted to produce improvements in muscle contraction when stimulation was on.
LESSONS
VSS appears to be safe, feasible, and well tolerated. VSS, as compared to standard-of-care therapy for SCI, can be used in conjunction with physical therapy and may lead to improvements in motor function.
Abstract: Transcutaneous Spinal Stimulation (TSS) is a promising rehabilitative intervention to restore motor function and coordination for individuals with spinal cord injury (SCI). This paper explores the potential for robotic assessment of the effects of TSS delivered to the cervical spinal cord. We used a four degree-of-freedom exoskeleton to measure the torque response of upper limb joints during stimulation, while simultaneously recording surface electromyography (sEMG). We show that site-specific effects of TSS are manifested not only by modulation of the amplitude of spinally evoked motor potentials in upper limb muscles, but also by changes in torque generated by individual upper limb joints.
Abstract: Transcutaneous spinal stimulation (TSS) is emerging as a valuable tool for electrophysiological and clinical assessment. This study examines the recruitment patterns of upper limb motor pools through the delivery of TSS above and below a spinal lesion. In eight participants with tetraplegia due to cervical SCI, TSS was delivered to the cervical spinal cord, and spinally evoked motor potentials in upper limb muscles were characterized. The findings indicate that electrophysiological data acquired through TSS can offer insights into the extent of upper limb functional asymmetry, disruptions in neural pathways, and changes in motor control following SCI.
Abstract: This study investigates the combinatorial effects of task-specific hand grip training and noninvasive TSS to enhance hand motor output after paralysis. Four participants with cervical SCI and two participants with cerebral stroke were recruited. The study demonstrated that combined task-specific hand grip training and cervical TSS targeting the motor pools of distal muscles in the upper limb resulted in significant improvements in maximum hand grip strength.
Abstract: Transcutaneous spinal stimulation (TSS) is a promising approach to restore upper-limb functions after spinal cord injury (SCI) in humans. This study demonstrates the selectivity of recruitment of individual upper-limb motor pools during cervical TSS using different electrode placements. The findings suggest that an arrangement of electrodes targeting specific upper-limb motor pools may result in superior efficacy, restoring more diverse motor activities after neurological injuries and disorders, including severe SCI.
Abstract: This study explores the effects of cervical transcutaneous spinal stimulation (TSS) on upper limb movements using a robotic exoskeleton. The effects of cutaneous TSS were observed by measuring the holding torque required by the exoskeleton to keep a user’s arm in a neutral position. The study identifies differences in resultant action based on the location of the stimulation electrodes with respect to the dorsal roots of the spinal cord.
Neuromodulation of spinal networks can improve motor control after spinal cord injury (SCI). The objectives of this study were to (1) determine whether individuals with chronic paralysis can stand with the aid of non-invasive electrical spinal stimulation with their knees and hips extended without trainer assistance, and (2) investigate whether postural control can be further improved following repeated sessions of stand training. Using a double-blind, balanced, within-subject cross-over, and sham-controlled study design, 15 individuals with SCI of various severity received transcutaneous electrical spinal stimulation to regain self-assisted standing. The primary outcomes included qualitative comparison of need of external assistance for knee and hip extension provided by trainers during standing without and in the presence of stimulation in the same participants, as well as quantitative measures, such as the level of knee assistance and amount of time spent standing without trainer assistance. None of the participants could stand unassisted without stimulation or in the presence of sham stimulation. With stimulation all participants could maintain upright standing with minimum and some (n = 7) without external assistance applied to the knees or hips, using their hands for upper body balance as needed. Quality of balance control was practice-dependent, and improved with subsequent training. During self-initiated body-weight displacements in standing enabled by spinal stimulation, high levels of leg muscle activity emerged, and depended on the amount of muscle loading. Our findings indicate that the lumbosacral spinal networks can be modulated transcutaneously using electrical spinal stimulation to facilitate self-assisted standing after chronic motor and sensory complete paralysis.
Despite autonomic dysfunction after spinal cord injury (SCI) being the major cause of death and a top health priority, the clinical management options for these conditions are limited to drugs with delayed onset and nonpharmacological interventions with equivocal effectiveness. We tested the capacity of electrical stimulation, applied transcutaneously over the spinal cord, to manage autonomic dysfunction in the form of orthostatic hypotension after SCI. We assessed beat-by-beat blood pressure (BP), stroke volume, and cardiac contractility (dP/dt; Finometer), as well as cerebral blood flow (transcranial Doppler) in 5 individuals with motor-complete SCI (4 cervical, 1 thoracic) during an orthostatic challenge with and without transcutaneous electrical stimulation applied at the TVII level. During the orthostatic challenge, all individuals experienced hypotension characterized by a 37 ± 4 mm Hg decrease in systolic BP, a 52 ± 10% reduction in cardiac contractility, and a 23 ± 6% reduction in cerebral blood flow (all p < 0.05), along with severe self-reported symptoms. Electrical stimulation completely normalized BP, cardiac contractility, cerebral blood flow, and abrogated all symptoms. Noninvasive transcutaneous electrical spinal cord stimulation may be a viable therapy for restoring autonomic cardiovascular control after SCI.
We reported previously that both transcutaneous electrical spinal cord stimulation and direct pressure stimulation of the plantar surfaces of the feet can elicit rhythmic involuntary step-like movements in noninjured subjects with their legs in a gravity-neutral apparatus. The present experiments investigated the convergence of spinal and plantar pressure stimulation and voluntary effort in the activation of locomotor movements in uninjured subjects under full body weight support in a vertical position. For all conditions, leg movements were analyzed using electromyographic (EMG) recordings and optical motion capture of joint kinematics. Spinal cord stimulation elicited rhythmic hip and knee flexion movements accompanied by EMG bursting activity in the hamstrings of 6/6 subjects. Similarly, plantar stimulation induced bursting EMG activity in the ankle flexor and extensor muscles in 5/6 subjects. Moreover, the combination of spinal and plantar stimulation exhibited a synergistic effect in all six subjects, eliciting greater motor responses than either modality alone. While the motor responses to spinal vs. plantar stimulation seems to activate distinct but overlapping spinal neural networks, when engaged simultaneously, the stepping responses were functionally complementary. As observed during induced (involuntary) stepping, the most significant modulation of voluntary stepping occurred in response to the combination of spinal and plantar stimulation. In light of the known automaticity and plasticity of spinal networks in absence of supraspinal input, these findings support the hypothesis that spinal and plantar stimulation may be effective tools for enhancing the recovery of motor control in individuals with neurological injuries and disorders.
The present prognosis for the recovery of voluntary control of movement in patients diagnosed as motor complete is generally poor. Herein we introduce a novel and noninvasive stimulation strategy of painless transcutaneous electrical enabling motor control and a pharmacological enabling motor control strategy to neuromodulate the physiological state of the spinal cord. This neuromodulation enabled the spinal locomotor networks of individuals with motor complete paralysis for 2-6 years American Spinal Cord Injury Association Impairment Scale (AIS) to be re-engaged and trained. We showed that locomotor-like stepping could be induced without voluntary effort within a single test session using electrical stimulation and training. We also observed significant facilitation of voluntary influence on the stepping movements in the presence of stimulation over a 4-week period in each subject. Using these strategies we transformed brain-spinal neuronal networks from a dormant to a functional state sufficiently to enable recovery of voluntary movement in five out of five subjects. Pharmacological intervention combined with stimulation and training resulted in further improvement in voluntary motor control of stepping-like movements in all subjects. We also observed on-command selective activation of the gastrocnemius and soleus muscles when attempting to plantarflex. At the end of 18 weeks of weekly interventions the mean changes in the amplitude of voluntarily controlled movement without stimulation was as high as occurred when combined with electrical stimulation. Additionally, spinally evoked motor potentials were readily modulated in the presence of voluntary effort, providing electrophysiological evidence of the re-establishment of functional connectivity among neural networks between the brain and the spinal cord.
Locomotor behavior is controlled by specific neural circuits called central pattern generators primarily located at the lumbosacral spinal cord. These locomotor-related neuronal circuits have a high level of automaticity; that is, they can produce a “stepping” movement pattern also seen on electromyography (EMG) in the absence of supraspinal and/or peripheral afferent inputs. These circuits can be modulated by epidural spinal-cord stimulation and/or pharmacological intervention. Such interventions have been used to neuromodulate the neuronal circuits in patients with motor-complete spinal-cord injury (SCI) to facilitate postural and locomotor adjustments and to regain voluntary motor control. Here, we describe a novel non-invasive stimulation strategy of painless transcutaneous electrical enabling motor control (pcEmc) to neuromodulate the physiological state of the spinal cord. The technique can facilitate a stepping performance in non-injured subjects with legs placed in a gravity-neutral position. The stepping movements were induced more effectively with multi-site than single-site spinal-cord stimulation. From these results, a multielectrode surface array technology was developed. Our preliminary data indicate that use of the multielectrode surface array can fine-tune the control of the locomotor behavior. As well, the pcEmc strategy combined with exoskeleton technology is effective for improving motor function in paralyzed patients with SCI. The potential impact of using pcEmc to neuromodulate the spinal circuitry has significant implications for furthering our understanding of the mechanisms controlling locomotion and for rehabilitating sensorimotor function even after severe SCI.
Transcutaneous and epidural electrical spinal cord stimulation techniques are becoming more valuable as electrophysiological and clinical tools. Recently, we observed selective activation of proximal and distal motor pools during epidural spinal stimulation. In the present study, we hypothesized that the characteristics of recruitment curves obtained from leg muscles will reflect a relative preferential activation of proximal and distal motor pools based on their arrangement along the lumbosacral enlargement. The purpose was to describe the electrophysiological responses to transcutaneous stimulation in leg muscles innervated by motoneurons from different segmental levels. Stimulation delivered along the rostrocaudal axis of the lumbosacral enlargement in the supine position resulted in a selective topographical recruitment of proximal and distal leg muscles, as described by threshold intensity, slope of the recruitment curves, and plateau point intensity and magnitude. Relatively selective recruitment of proximal and distal motor pools can be titrated by optimizing the site and intensity level of stimulation to excite a given combination of motor pools. The slope of the recruitment of particular muscles allows characterization of the properties of afferents projecting to specific motoneuron pools, as well as to the type and size of the motoneurons. The location and intensity of transcutaneous spinal electrical stimulation are critical to target particular neural structures across different motor pools in investigation of specific neuromodulatory effects. Finally, the asymmetry in bilateral evoked potentials is inevitable and can be attributed to both anatomical and functional peculiarities of individual muscles or muscle groups.
Predictions about one’s own action capabilities as well as the action capabilities of others are thought to be based on a simulation process involving linked perceptual and motor networks. Given the central role of motor experience in the formation of these networks, one’s present motor capabilities are thought to be the basis of their perceptual judgments about actions. However, it remains unknown whether the ability to form these action possibility judgments is affected by performance related changes in the motor system. To determine if judgments of action capabilities are affected by long-term changes in one’s own motor capabilities, participants with different degrees of upper-limb function due to their level (cervical vs. below cervical) of spinal cord injury (SCI) were tested on a perceptual-motor judgment task. Participants observed apparent motion videos of reciprocal aiming movements with varying levels of difficulty. For each movement, participants determined the shortest movement time (MT) at which they themselves and a young adult could perform the task while maintaining accuracy. Participants also performed the task. Analyses of MTs revealed that perceptual judgments for participant’s own movement capabilities were consistent with their actual performance- people with cervical SCI had longer judged and actual MTs than people with below cervical SCI. However, there were no between-group differences in judged MTs for the young adult. Although it is unclear how the judgments were adjusted (altered simulation vs. threshold modification), the data reveal that people with different motor capabilities due to SCI are not completely biased by their present capabilities and can effectively adjust their judgments to estimate the actions of others.
Methods: Ulnar nerve stimulation and transcutaneous electrical spinal stimulation were used in a condition-test paradigm to evaluate the presence of interlimb connections linking the cervical and lumbosacral spinal segments in non-injured (n=15) and spinal cord injured (SCI) (n=18) participants.
Results: Potentiation of spinally evoked motor responses (sEMRs) by ulnar nerve conditioning was observed in 7/7 SCI participants with volitional leg muscle activation, and in 6/11 SCI participants with no volitional activation. Of these six, conditioning of sEMRs was present only when the neurological level of injury was rostral to the ulnar innervation entry zones.
Conclusions: Descending modulation of lumbosacral motor pools via interlimb projections may exist in SCI participants despite the absence of volitional leg muscle activation.
Significance: Evaluation of sub-clinical, spared pathways within the spinal cord after SCI may provide an improved understanding of both the contributions of different pathways to residual function, and the mechanisms of plasticity and functional motor recovery following rehabilitation..
Methods: Center of pressure displacement and electromyograms from the soleus and tibialis anterior were recorded in seven individuals with multiple sclerosis during standing without and with transcutaneous spinal stimulation. Center of pressure and muscle activity measures were calculated and compared between no stimulation and transcutaneous spinal stimulation conditions. The relationship between the center of pressure displacement and electromyograms was quantified using cross-correlation analysis.
Results: For transcutaneous spinal stimulation, postural stability was significantly improved during standing with eyes closed: the time- and frequency-domain measures obtained from the anterior-posterior center of pressure fluctuation decreased and increased, respectively, and the tibialis anterior activity was lower compared to no stimulation. Conversely, no differences were found between no stimulation and transcutaneous spinal stimulation when standing with eyes open.
Conclusion: Following multiple sclerosis, transcutaneous spinal stimulation improved postural stability during standing with eyes closed, presumably by catalyzing proprioceptive function. Future work should confirm underlying mechanisms and explore the clinical value of transcutaneous spinal stimulation for individuals with multiple sclerosis.
Methods: An initial 100-s baseline period was followed by 50-s cold stimulation periods. Stretch reflex of the right soleus muscle was elicited for 10-s intervals, while cold stimulation was applied to the left thigh.
Results: Peak-to-peak amplitude of the stretch reflex increased significantly during cold stimulation up to 127 ± 21% of the baseline in the able-bodied group (n=9, P<0.01). Similarly, stretch reflex increased up to 125 ± 11% in a group with injury level at or below thoracic 10 (n=4), although this increase was not significant. On the other hand, stretch reflex decreased significantly down to 78 ± 20% in a group with injury level at or above thoracic 6 (n=8, P<0.05).
Conclusions: Effect of afferent inputs induced by cold stimulation on stretch reflex modulation is different depending on the extent of central nervous systems participating in the modulation.
Significance: Our findings provide a better understanding of some basic changes in afferent-efferent spinal reflex pathways which are probably not monosynaptic in nature.
Functional electrical stimulation (FES) involves electrically stimulating the neuromuscular system to generate skeletal muscle contractions in paralyzed muscles. Several new FES applications have been proposed that require closed-loop control systems. Co-contraction of antagonist muscle groups has been postulated as a promising approach for closed-loop control of FES systems. However, this control approach has not yet been used in practical FES applications, in part due to a lack of information concerning how able-bodied subjects use co-contraction of antagonist muscles during standard control tests such as unit step and sinusoidal responses. The purpose of this work is to elucidate how able-bodied individuals use co-contraction by analyzing the EMG activity of antagonist muscles during voluntary knee extension against gravity. The results clearly demonstrate that able-bodied subjects use a co-contraction strategy when executing standard control performance tests, and strengthen the argument for using a co-contraction strategy for closed-loop FES control algorithms. These data will inform the development of new and effective controllers for FES applications.
Methods: SDSS was delivered through four active electrodes applied to the plantarflexors, sending a stimulation pulse to each electrode one after another with 90° phase shift between successive electrodes. In the first experiment, the amount of exerted ankle torque and the muscle contractile properties were investigated during a 3 min fatiguing stimulation. In the second experiment, muscle twitch potentials with SDSS and SES stimulation electrode setups were compared using the array-arranged EMG.
Results: The results demonstrated negligible torque decay during SDSS in contrast to considerable torque decay during SES. Moreover, small changes in the muscle contractile properties during the fatiguing stimulation using SDSS were observed, while slowing of muscle contraction and relaxation was observed during SES. Further, the amplitude of the M-waves at each muscle portion was dependent on the location of the stimulation electrodes during SDSS.
Conclusion: We conclude that SDSS is more effective in reducing muscle fatigue compared to SES, and the reason is that different sets of muscle fibers are activated alternatively by different electrodes.
Setting: National Rehabilitation Center for Persons with Disabilities, Tokorozawa, Japan.
Methods: Six participants with chronic motor and sensory incomplete SCI who were able to stand for at least 5 min without any form of assistive device performed the VBT, 3 days per week, for a total of 12 sessions. During the training, participants stood on a force platform and were instructed to shift their center of pressure in the indicated directions as represented by a cursor on a monitor. The performance and the rate of learning were monitored throughout the training period. Before and after the program, static and dynamic stability was assessed.
Results: All participants showed substantial improvements in the scores, which varied between 236±94 and 130±14% of the initial values for different exercises. The balance performance during training-irrelevant tasks was significantly improved: for example, the area inside the stability zone after the training reached 221±86% of the pre-training values.
Conclusion: Postural control can be enhanced in individuals with incomplete SCI using VBT. All participants showed substantial improvements during standing in both game performance and training-irrelevant tasks after the VBT.
Objective: To extend the previous findings and to prove feasibility of the method by exploring the fatigue-reducing ability of SDSS for lower limb muscle groups in the able-bodied population, as well as in individuals with spinal cord injury (SCI).
Methods: SDSS was delivered through 4 active electrodes applied to the knee extensors and flexors, plantarflexors, and dorsiflexors, sending a stimulation pulse to each electrode one after another with 90° phase shift between successive electrodes. Isometric ankle torque was measured during fatiguing stimulations using SDSS and conventional single active electrode stimulation lasting 2 minutes.
Results: We demonstrated greater fatigue-reducing ability of SDSS compared with the conventional protocol, as revealed by larger values of fatigue index and/or torque peak mean in all muscles except knee flexors of able-bodied individuals, and in all muscles tested in individuals with SCI.
Conclusions: Our study has revealed improvements in fatigue tolerance during transcutaneous neuromuscular electrical stimulation using SDSS, a stimulation strategy that alternates activation of subcompartments of muscles. The SDSS protocol can provide greater stimulation times with less decrement in mechanical output compared with the conventional protocol.
Design: Case series.
Methods: Seven adult men with chronic (≥2 years), thoracic motor complete (AIS A-B) SCI completed a 40-week course of thrice-weekly intermittent PS-WBV therapy, in a flexed knee posture (160°), for 45 minutes per session at a frequency of 45 Hz and 0.6-0.7 mm displacement using the WAVE(®) Pro Plate, with an integrated EasyStand™ standing frame. EMG was measured in major lower extremity muscles to represent muscle activity during PS-WBV. The cross-sectional area and density of the calf muscles were measured using peripheral quantitative computed tomography at the widest calf cross-section (66% of the tibia length) at pre- and post-intervention. All measured variables were compared between the pre- and post-intervention measurements to assess change after the PS-WBV intervention.
Results: PS-WBV acutely induced EMG activity in lower extremity muscles of SCI subjects. No significant changes in lower extremity EMG activity, muscle cross-sectional area, or density were observed following the 40-week intervention.
Conclusions: Although acute exposure to PS-WBV can induce electrophysiological activity of lower extremity muscles during PS in men with motor complete SCI, the PS-WBV intervention for 40 weeks was not sufficient to result in enhanced muscle activity, or to increase calf muscle cross-sectional area or density.
Methods: Ten male subjects participated in the study, six able-bodied and four with chronic SCI. Two different manufacturers’ vibration platforms (WAVE(®) and Juvent™) were evaluated. The effects of vibration amplitude (0.2, 0.6 or 1.2 mm), vibration frequency (25, 35, or 45 Hz), and subject posture (knee angle of 140°, 160°, or 180°) on lower extremity EMG activation were determined (not all combinations of parameters were possible on both platforms). A novel signal processing technique was proposed to estimate the power of the EMG waveform while minimizing interference and artifacts from the plate vibration.
Results: WBV can elicit EMG activity among subjects with chronic SCI, if appropriate vibration parameters are employed. The amplitude of vibration had the greatest influence on EMG activation, while the frequency of vibration had lesser but statistically significant impact on the measured lower extremity EMG activity.
Conclusion: These findings suggest that WBV with appropriate parameters may constitute a promising intervention to treat musculoskeletal degradation after chronic SCI.